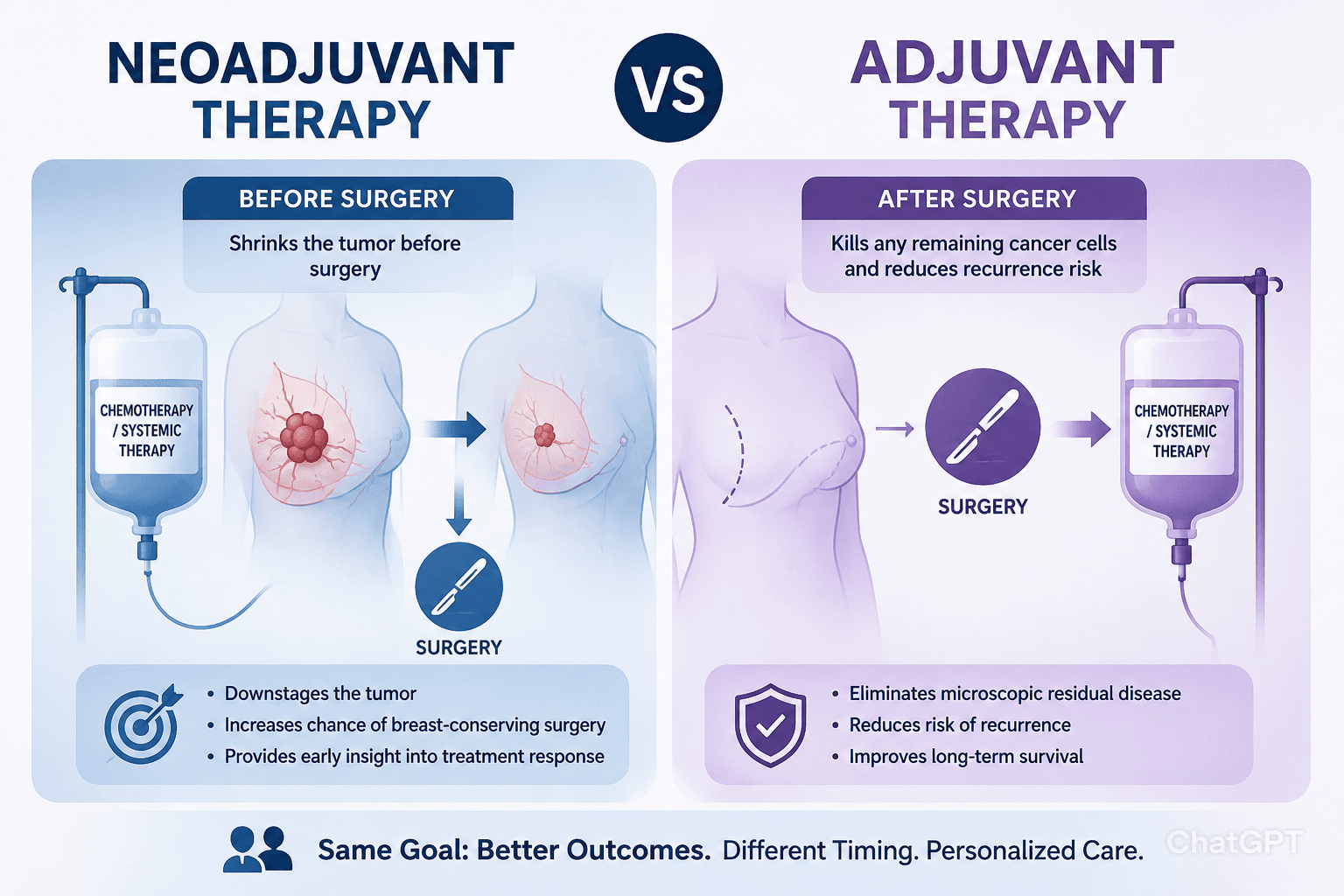
Neoadjuvant therapy is treatment given before the main surgical procedure, while adjuvant therapy is the treatment that follows surgery to eliminate any remaining microscopic cancer. Both therapies aim to improve survival, but they differentiate in timing, goals, and the way they affect the tumor and surrounding tissue.
Choosing the right therapy for cancer treatment in Kolkata depends on cancer type, stage, and patient health. Oncologists evaluate whether shrinking the tumor first or securing the surgical field later will give the best chance of cure.
Key Takeaways
- Neoadjuvant therapy can shrink tumors up to 40% before surgery, makingbreast‑conserving surgery possible for many patients (CDC, 2022).
- Adjuvant therapy reduces the risk of recurrence by targeting micrometastatic disease after the tumor is removed.
- Both neoadjuvant and adjuvant approaches are standard for breast cancer, lung cancer, ovarian cancer, and certain head‑and‑neck cancers.
- Clinical trials show that patients receiving neoadjuvant chemotherapy plus immunotherapy have a 15% higher pathologic complete response rate compared with chemotherapy alone in some cancers
- Side‑effects such as nausea, fatigue, and hair loss are similar for both approaches, but timing can affect a patient’s ability to work during treatment.
What Is Neoadjuvant Therapy?
Neoadjuvant therapy includes chemotherapy, radiation therapy, hormone therapy, or targeted therapies. The primary goal is to shrink the tumor so that surgery can be less extensive. In breast cancer, a successful neoadjuvant regimen can turn a planned mastectomy into a lumpectomy, making the breast easier to remove and preserving more tissue.
Neoadjuvant therapies also provide early information about how the cancer cell population responds to treatment. Pathologists can assess the degree of tumor regression, which helps predict long‑term outcomes. For example, patients whose tumors achieve a complete pathological response often enjoy higher survival rates.
In addition to shrinking the primary mass, neoadjuvant treatment may eradicate micrometastasis, reducing the chance that remaining cancer cells cause a future relapse. This is particularly valuable in aggressive subtypes such as HER2‑positive breast cancer where targeted therapy with pertuzumab or trastuzumab is combined with chemotherapy.
What Is Adjuvant Therapy?
Adjuvant therapy is administered after the surgical removal of the tumor. Its purpose is to eradicate any residual disease that could lead to a risk of recurrence. Common modalities of Adjuvant therapy include chemotherapy, radiation therapy, hormone therapy, and newer immunotherapy agents.
In colon cancer and lung cancer, adjuvant chemotherapy has been shown to improve five‑year survival by up to 10% (National Cancer Institute). Hormone therapy, such as tamoxifen for estrogen‑receptor‑positive breast cancer, can reduce the risk of distant metastasis for up to ten years.
Adjuvant therapy may also incorporate targeted therapies like pembrolizumab for high‑risk melanoma, or EGFR inhibitors for non‑small‑cell lung cancer. These treatments are tailored based on molecular profiling, a cornerstone of personalized medicine in modern oncology.
Comparing Neoadjuvant and Adjuvant Approaches
| Aspect | Neoadjuvant Therapy | Adjuvant Therapy |
| Timing | Before surgery | After surgery |
| Primary Goal | Shrink tumor, make surgery easier | Eliminate remaining cancer cells |
| Common Modalities | Chemo, radiation, hormone, targeted | Chemo, radiation, hormone, immunotherapy |
| Effect on Surgical Choice | May convert mastectomy to lumpectomy; makes tumor easier to remove | Does not change surgical plan |
| Assessment of Efficacy | Pathologic response after resection | Imaging and tumor marker surveillance |
| Typical Cancers | Breast, rectal, esophageal, lung | Colorectal, breast, prostate, melanoma |
How We Assess If Neoadjuvant Treatment Is Effective
Effectiveness is measured by radiologic reduction in size, pathology reports showing tumor regression, and biomarkers such as Ki‑67. A complete pathological response correlates with lower recurrence rates and better overall survival.
Clinical Applications and Decision‑Making
Choosing between neoadjuvant and adjuvant therapy depends on cancer stage, molecular profile, and patient preferences. Breast cancer patients with large tumors or aggressive subtypes often receive neoadjuvant chemotherapy to shrink the mass before surgery, potentially allowing a breast‑conserving lumpectomy. For early‑stage disease, adjuvant therapy may be sufficient.
In lung cancer, neoadjuvant chemotherapy along with immunotherapy can downstage a tumor, making it resectable for patients who would otherwise be inoperable. Meanwhile, adjuvant chemotherapy after a lobectomy is standard for stage II–III non‑small‑cell lung cancer to improve survival.
Rectal cancer treatment protocols frequently use neoadjuvant radiation for rectal tumors to increase the chance of sphincter‑preserving surgery. After resection, adjuvant chemotherapy targets any remaining cancer cells.
For patients living in Kolkata with hormone‑responsive disease, hormone therapy may be given as an adjuvant to block estrogen signaling, reducing the risk of new cancer cells forming.
Emerging immunotherapy trials show that combining neoadjuvant immune checkpoint inhibitors with chemotherapy can boost response rates across several tumor types, including melanoma and bladder cancer.
Frequently Asked Questions
Which is better, adjuvant or neoadjuvant therapy?
Neither is universally superior; the optimal choice depends on tumor size, stage, and biology. Neoadjuvant therapy is preferred when shrinking the tumor can make surgery less invasive, while adjuvant therapy is essential for eradicating microscopic disease after resection.
What are the 7 main types of chemotherapy?
The major categories include alkylating agents, antimetabolites, anthracyclines, taxanes, vinca alkaloids, platinum compounds, and topoisomerase inhibitors. Each class works by disrupting specific steps in cancer cell replication.
What cancers use neoadjuvant therapy?
Neoadjuvant approaches are common in breast, lung, rectal, esophageal, and pancreatic cancers. They are also employed in selected cases of melanoma and head‑and‑neck cancers to improve surgical outcomes.
Which cancers need adjuvant chemotherapy?
Adjuvant chemotherapy is standard after surgery for stage II–III colon, breast, lung, ovarian, endometrial and certain sarcomas. It targets residual disease and lowers the risk of recurrence.
Can you work during chemotherapy?
Many patients continue employment, especially when treatment is outpatient and side effects are manageable. Adjusted schedules, supportive care, and flexible employers improve the ability to maintain work during therapy.
Neoadjuvant and adjuvant therapies each play a crucial role in modern cancer care. By tailoring treatment timing to the specific disease and patient, oncologists can maximize tumor control, preserve organ function, and improve survival.
For personalized guidance on whether neoadjuvant or adjuvant treatment is right for you, consult a qualified oncology specialist in Kolkata. Learn more about comprehensive cancer care options at Dr. Sandip Ganguly’s Cancer Treatment Center, Kolkata.